As I listen to the post-Dobbs public discourse about abortion and women’s health, I am reminded of the three years I spent working at a mission hospital in rural Kenya as the only obstetrician-gynecologist for over 300,000 people. Having joined my specialty in part because I was compelled by the complexity of caring for pregnant women and their pre-born children at the same time, I knew I would face unique challenges in Kenya. What I did not fully appreciate was the extent to which a lack of resources would compound the challenge. Our hospital often lacked the medical supplies, medications, and blood necessary to treat pregnant women or their premature babies in medical emergencies. One time, when operating on a woman who was hemorrhaging, I had to scrub out of surgery, donate my own blood, and scrub back in to prevent her from dying from hemorrhagic shock.
Now that I am back in the U.S. serving as an OB-GYN hospitalist in Fort Wayne, Indiana, I am finding that caring for mothers and pre-born children at the same time is just as much a challenge here as it was in Kenya—but for different reasons. In Kenya, we lacked resources. In the U.S., we lack the will. Having had abortion as a major part of our culture for fifty years, many do not view the pre-born child as inherently valuable or worth caring for. Even many Christians feel hesitant about offering them the same legal protections as everyone else who was made in God’s image.
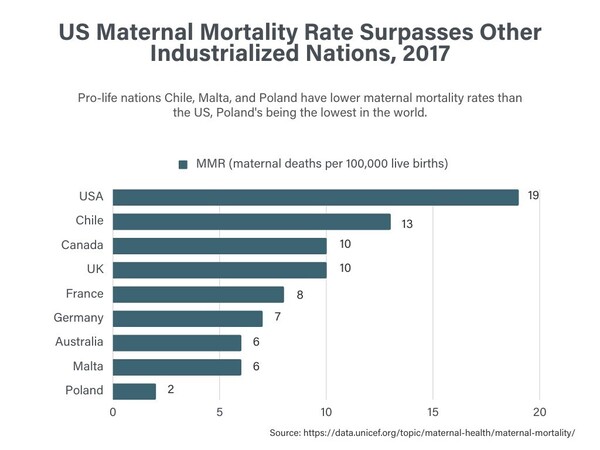
Today, many of those within the Church who feel uncertain about banning abortion often cite concerns that such bans will harm the overall quality of women’s healthcare. But my experience in Kenya has shown me what high-quality, lifesaving reproductive healthcare requires—and it does not include elective abortion. Just look at the countries that have banned abortion in the past few decades. Chile enacted an abortion ban in 1989, and this law had zero effect on its steadily declining maternal mortality rate (MMR). Today, Chile has the lowest MMR in South America. Two countries with some of the lowest MMRs in the world—Malta and Poland—both have abortion bans as well. In the United States, Catholic and other religious hospitals and pro-life physicians have practiced without abortion throughout the duration of the Roe era and were still able to offer lifesaving care to women.
I completed my residency at a hospital that does not perform abortions, and I was able to care for women facing all kinds of medical emergencies in a way that respected not only their lives, but also those of their pre-born children. Additionally, we have had nearly unfettered access to abortion in the U.S. since 1973, including to second and third-trimester abortions, and yet our maternal mortality rate continues to worsen and remains the worst in the developed world. Women in the U.S. die from pregnancy-related complications at a rate 2 to 3 times higher than in European countries—the majority of which restrict abortion to the first trimester only (see: Figure 1 below).
Abolishing abortion and offering top-quality medical care to women are possible to do simultaneously. Perhaps if many Christians today understood this they would feel less hesitant to support the pro-life values that the Church has held from the beginning. The Church’s two-thousand-year legacy of opposing abortion stems from the recognition that the practice violates the Commandment—“you shall not murder”—and the principle that all people, both born and pre-born, are created in the image of God and therefore have infinite worth and value.
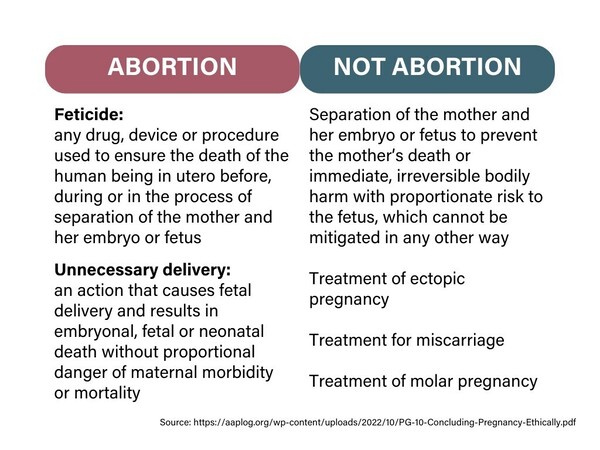
Induced abortion is defined by several medical bodies as a procedure that ends a pregnancy in such a way that it does not result in a live birth—that is, by intentionally ending the life of the pre-born human being (intentional feticide). As an OB-GYN who is also a Christian and so sees the image of God in every pre-born child, such a practice is unconscionable. After all, pre-born babies are just as much our patients as their pregnant mothers, and intentionally killing one of our patients is neither ethical nor good medical care. Even OB-GYNs who do not consider themselves pro-life understand that abortion ends the life of one of their patients and is thus antithetical to our oath as physicians. That is why more than 90% of practicing OB-GYNs do not perform elective abortions.
Yet, we have all treated women facing pregnancy complications that may threaten their lives. You have probably seen many of these conditions mentioned in the news—miscarriage, ectopic pregnancy, premature preterm rupture of pregnancy (PPROM), placental abruption, just to name a few. But abortion is not necessary to address these conditions, nor would the treatments for these conditions be prosecuted under any state-level abortion ban to date.
Perhaps one of the most egregious justifications used for opposing abortion restrictions is the claim that women will not be able to receive care for miscarriages. A miscarriage occurs when the embryo or fetus passes away spontaneously. It is a tragic circumstance for any family to experience and if the mother’s body does not deliver the baby on its own, medical intervention is needed to prevent complications. Treatment methods for a miscarriage can include the same procedures used in an abortion—the use of the drug misoprostol, dilation and curettage (D&C), and dilation and evacuation (D&E). The intent of the procedure makes all the difference here: a D&C for a miscarriage is the removal of a pre-born child who has already died; the same procedure for an elective abortion kills a living, potentially pain-capable, human being through dismemberment. It is like the difference between performing a tracheostomy to help someone breathe and doing so to kill them. One is life-saving medicine; the other is murder. The tools and procedures themselves are not the issues; the intent is.
But what if the pre-born child is still alive when the mother faces a life-threatening situation? One example of this is in the case of an ectopic pregnancy. This is when an embryo is implanted outside of the uterine cavity; usually, it is in the fallopian tube, but may also be in the ovary, cervix, or elsewhere. None of these locations are suitable to hold a growing baby, which means that the mother is at great risk for life-threatening hemorrhage as the pregnancy grows. This represents a legitimately life-threatening situation for the mother and one in which the pre-born child, unfortunately, has no chance at survival.
Every physician recognizes this and, regardless of their position on elective abortion, would not hesitate to treat it. In most cases, the pre-born child has already passed by the time the ectopic pregnancy is diagnosed, however even in the rare cases where a heartbeat is still present, treating an ectopic pregnancy is not the same as an abortion. Even Planned Parenthood’s website admitted as much, at least before they removed the statement in the wake of the Dobbs decision. The reason for this is clear—again, there is a difference in intent. In such an emergency, the only way to save the mother’s life is to separate her from her pre-born child. As pro-life physicians, we are pro- the life of the mother and pro- the life of the baby—we save those that we can save. If we had the option of saving both mother and baby in this situation we would; instead, we must make a decision between saving the mother and losing baby or losing both.
There are other complications that can arise during a pregnancy for which the only way to save the mother’s life is to separate her and her baby as soon as possible. If this occurs after the point at which a pre-born baby can survive outside of the womb (roughly 22 to 23 weeks gestation given today’s medical technology), then the decision is obvious—a doctor can simply deliver the baby and treat the mother and the baby separately. Abortion is completely unnecessary. In fact, it may take several days to complete an abortion procedure that requires cervical preparation. In a true emergency, this would waste precious time compared to an emergency C-section that can be completed in minutes and affords both the mother and the baby the best chances of survival.
If, however, the emergency arises prior to the point of viability outside the womb, the doctor will still have to deliver the baby despite knowing that in all likelihood the baby will not survive the procedure. As with an ectopic pregnancy, this is a tragic choice that a doctor must make together with the patient in order to save her life. However, as with an ectopic pregnancy, the lack of intention to kill means that this treatment is not the same as an abortion (see: Figure 2 below).
Finally, even among Christians, cases in which the pre-born baby has been diagnosed with a potentially life-limiting diagnosis are often used to justify elective abortion. From a medical perspective, abortion is entirely unnecessary in these situations. Many will ask, “Is it compassionate to make women carry a pregnancy to term when they know the child will not live for very long or could potentially suffer?” I think it is imperative that we shift our thinking on this question. A diagnosis made when a child is still in utero is no different than one made after birth. Tragically, children are sometimes diagnosed with terminal illnesses after birth—cancer, heart defects, even conditions that could have potentially been caught in utero. Yet we would never consider intentionally ending the life of a child who has already been born upon the receipt of a life-limiting diagnosis.
Instead, physicians fight to preserve the lives of these children, or offer them hospice care when that is not possible. There is no reason not to do the same for pre-born children. In fact, hospitals across the country do offer perinatal hospice as an option to parents who choose to move forward with a pregnancy after a life-limiting diagnosis. With this option, physicians are able to respect the life and dignity of the child regardless of how short that child’s life might be and parents receive dedicated time to love, hold, and say goodbye to their child. Studies have shown that perinatal hospice yields better mental health outcomes for grieving parents. As Christians who believe that every human being was knitted together by God in his or her mother’s womb (Psalm 139), we should advocate for the option that best recognizes the inherent dignity of every person regardless of age or ability level.
Another reason to reject abortion due to potential fetal anomaly is that sometimes, physicians are wrong in their diagnosis. Recent research on the accuracy (or lack thereof) and misuse of prenatal genetic screening tests has made that clear. Often parents feel pressured into an abortion based on an inaccurate diagnosis. But even if a diagnosis is correct, doctors’ predictions about a child’s length or quality of life can be wrong. My goddaughter, for example, was diagnosed in-utero with hydrops fetalis and cystic hygroma, two conditions that together offered her a 5% chance of living to birth and a 0% chance of surviving outside the womb. However, her mother chose to move forward with the pregnancy, and today, that zero-percent-chance baby is nine years old and brings her family untold joy. Christians should recognize that God often has different plans than what may seem obvious to us, and we should make room for them.
Having practiced obstetrics for 18 years without once performing an elective abortion, I know that the tragic stories circulating recently about women receiving subpar treatment in states that have restricted abortion access could have been avoided. Every pregnant woman and her baby deserve the highest quality medical care that physicians can offer.
Christians should not fear that abortion restrictions inherently threaten women’s lives. This is a narrative pushed to intentionally sow confusion about the definition of abortion and exploit women’s heartbreaking medical experiences in order to promote and normalize abortion at any stage of pregnancy, for any reason. In this post-Roe world, I hope that the Church gains perspective on the type of healthcare that pregnant women truly need to thrive. Medical evidence reveals what is necessary to offer high-quality care to pregnant women; it is exactly the things we lacked at the missionary hospital in Kenya: accessible prenatal care, antibiotics, blood to treat hemorrhages, and access to skilled birth attendants. Notice that abortion does not make this list. Efforts to market abortion as “care” or claims that it is an essential component of women’s healthcare are misguided at best, and intentionally misleading at worst. In fact, it is my firm belief that the medical field would be much better off without abortion.
As a pro-life physician, I am excited to build a world in which the image of God is recognized in every human being, born or pre-born. Far from harming women’s health, I foresee that this life-affirming change in our society will give rise to positive developments in reproductive healthcare. Without using abortion as a crutch to avoid dealing with the various root problems that cause women to choose to terminate pregnancies—from socio-economic challenges to mental health to life-limiting fetal diagnoses—healthcare providers will look for real solutions that promote life instead of ending it. I am proud to be a part of this post-Roe era and look forward to helping women and their families flourish in this new environment.